Quest Diagnostics 2015 Annual Report Download - page 27
Download and view the complete annual report
Please find page 27 of the 2015 Quest Diagnostics annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
 17
17 -
 18
18 -
 19
19 -
 20
20 -
 21
21 -
 22
22 -
 23
23 -
 24
24 -
 25
25 -
 26
26 -
 27
27 -
 28
28 -
 29
29 -
 30
30 -
 31
31 -
 32
32 -
 33
33 -
 34
34 -
 35
35 -
 36
36 -
 37
37 -
38
-
39
-
40
-
41
-
42
-
43
-
44
-
45
-
46
-
47
-
48
-
49
-
50
-
51
-
52
-
53
-
54
-
55
-
56
-
57
-
58
-
59
-
60
-
61
-
62
-
63
-
64
-
65
-
66
-
67
-
68
-
69
-
70
-
71
-
72
-
73
-
74
-
75
-
76
-
77
-
78
-
79
-
80
-
81
-
82
-
83
-
84
-
85
-
86
-
87
-
88
-
89
-
90
-
91
-
92
-
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
-
114
-
115
-
116
-
117
-
118
-
119
-
120
-
121
-
122
-
123
-
124
-
125
-
126
-
127
-
128
-
129
 |
 |
23
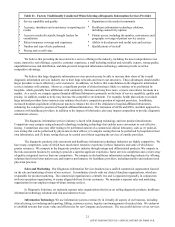
Our success in remaining a leading innovator in the diagnostic information services industry by continuing to
introduce new tests, technology and services will depend, in part, on our ability to license new and improved technologies on
favorable terms. Other companies or individuals, including our competitors, may obtain patents or other property rights on
tests or processes that we may be performing, particularly in such emerging areas as gene-based testing and other specialty
testing, that could prevent, limit or interfere with our ability to develop, perform or sell our tests or operate our business.
Employees. At December 31, 2015, we employed approximately 44,000 people. This total excludes employees of the
joint ventures where we do not have a majority ownership interest. We have no collective bargaining agreements with unions
covering employees in the United States, and we believe that our overall relations with our employees are good.
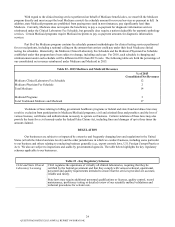
BILLING AND REIMBURSEMENT
Billing. We generally bill for diagnostic information services on a fee-for-service basis under one of two types of fee
schedules. These fees may be negotiated or discounted. The types of fee schedules are:
• “Client” fees charged to physicians, hospitals and institutions for which services are performed on a wholesale
basis and which are billed on a monthly basis.
• “Patient” fees charged to individual patients and certain third-party payers on a claim-by-claim basis.
Billing for diagnostic information services is very complicated, and we maintain compliance policies and procedures
for our billing. Patients, insurance companies, Medicare, Medicaid, physicians, hospitals, IDNs and employer groups all have
different billing requirements. Some billing arrangements require us to bill multiple payers, and there are several other factors
that complicate billing (e.g., disparity in coverage and information requirements among various payers; and incomplete or
inaccurate billing information provided by ordering clinicians). We incur additional costs as a result of our participation in
Medicare and Medicaid programs because diagnostic testing services are subject to complex, stringent and frequently
ambiguous federal and state laws and regulations, including those relating to coverage, billing and reimbursement.
Additionally, auditing for compliance with applicable laws and regulations as well as internal compliance policies and
procedures adds further cost and complexity to the billing process. Changes in laws and regulations could further complicate
our billing and increase our billing costs. CMS establishes procedures and continuously evaluates and implements changes to
the reimbursement process and requirements for coverage.
As an integral part of our billing compliance program, we investigate reported failures or suspected failures to comply
with federal and state healthcare reimbursement requirements. Any Medicare or Medicaid overpayments resulting from non-
compliance are reimbursed by us. As a result of these efforts, we have periodically identified and reported overpayments,
reimbursed the payers for overpayments and taken appropriate corrective action.
Our bad debt expense is primarily the result of the failure of patients to pay the portion of the receivable that is their
responsibility. In recent years, increased patient responsibility has adversely impacted our bad debt expense. To the extent that
health plans and other programs require greater levels of patient cost-sharing, this could negatively impact our bad debt
expense. We are taking, and plan to continue to take, steps to improve our patient collection experience.
The remainder of our bad debt expense is primarily due to missing or incorrect billing information on requisitions and
Advance Beneficiary Notices received from healthcare providers. In general, due to the nature of our business, historically we
have performed the requested testing and reported test results regardless of whether the billing information is correct or
complete. We subsequently attempt to contact the healthcare provider or patient to obtain any missing information and to
rectify incorrect billing information. Missing or incorrect information on requisitions complicates and slows down the billing
process, creates backlogs of unbilled requisitions and generally increases the aging of accounts receivable and bad debt
expense. The increased use of electronic ordering reduces the incidence of missing or incorrect information.
Government Coverage and Reimbursements. Government payers, such as Medicare and Medicaid, have taken steps
and are expected to continue to take steps to control the cost, utilization and delivery of healthcare services, including clinical
test services. Historically, most Medicare and Medicaid beneficiaries were covered under the traditional Medicare and
Medicaid programs administered by the federal government. Over the last several years, the federal government has continued
to expand its contracts with private health insurance plans for Medicare beneficiaries and has encouraged such beneficiaries to
switch from the traditional programs to the private programs, called “Medicare Advantage” programs. There has been growth
of health insurance providers offering Medicare Advantage programs and of beneficiary enrollment in these programs. In
recent years, in an effort to control costs, states also have mandated that Medicaid beneficiaries enroll in private managed care
arrangements.
QUEST DIAGNOSTICS 2015 ANNUAL REPORT ON FORM 10-K