United Healthcare 2015 Annual Report Download - page 71
Download and view the complete annual report
Please find page 71 of the 2015 United Healthcare annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
-
21
-
22
-
23
-
24
-
25
-
26
-
27
-
28
-
29
-
30
-
31
-
32
-
33
-
34
-
35
-
36
-
37
-
38
-
39
-
40
-
41
-
42
-
43
-
44
-
45
-
46
-
47
-
48
-
49
-
50
-
51
-
52
-
53
-
54
-
55
-
56
-
57
-
58
-
59
-
60
-
 61
61 -
 62
62 -
 63
63 -
 64
64 -
 65
65 -
 66
66 -
 67
67 -
 68
68 -
 69
69 -
 70
70 -
 71
71 -
 72
72 -
 73
73 -
 74
74 -
 75
75 -
 76
76 -
 77
77 -
 78
78 -
 79
79 -
 80
80 -
 81
81 -
82
-
83
-
84
-
85
-
86
-
87
-
88
-
89
-
90
-
91
-
92
-
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
 |
 |
Industry Tax at the beginning of the calendar year with a corresponding deferred cost that is amortized to
operating costs on the Consolidated Statements of Operations using a straight-line method of allocation over the
calendar year. The liability is recorded in accounts payable and accrued liabilities and the corresponding deferred
cost is recorded in prepaid expenses and other current assets on the Consolidated Balance Sheets. In September
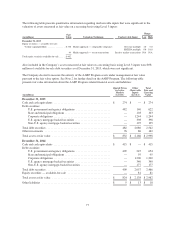
2015, the Company paid its full year 2015 Health Insurance Industry Tax of $1.8 billion. There was no liability
or asset related to the Health Insurance Industry Tax recorded as of both December 31, 2015 and 2014 as the
Health Insurance Industry Tax was paid in September of both years and the asset was fully expensed by each
year end.
Premium Stabilization Programs
Health Reform Legislation has included three programs designed to stabilize health insurance markets (Premium
Stabilization Programs): a permanent risk adjustment program; a temporary risk corridors program; and a
transitional reinsurance program (Reinsurance Program).
The risk-adjustment provisions apply to market reform compliant individual and small group plans in the
commercial markets. Under the program, each covered member is assigned a risk score based upon demographic
information and applicable diagnostic codes from the current year paid claims, in order to determine an average
risk score for each plan in a particular state and market risk pool. Generally, a plan with a risk score that is less
than the state’s average risk score will pay into the pool, while a plan with a risk score that is greater than the
state’s average will receive money from the pool. The temporary risk corridors provisions are intended to limit
the gains and losses of individual and small group qualified health plans. Plans are required to calculate the U.S.
Department of Health and Human Services (HHS) risk corridor ratio of allowable costs to the defined target
amount. Qualified health plans with ratios below 97% are required to make payments to HHS, while plans with
ratios greater than 103% expect to receive funds from HHS. The Reinsurance Program is a transitional three year
program through 2016 that is funded on a per capita basis from all commercial lines of business, including
insured and self-funded arrangements.
For the Premium Stabilization Programs, the Company records a receivable or payable as an adjustment to
premium revenue based on year-to-date experience when the amounts are reasonably estimable and collection is
reasonably assured. Final adjustments or recoverable amounts to the Premium Stabilization Programs are
determined by HHS in the year following the policy year.
Recently Issued Accounting Standards
In May 2014, the Financial Accounting Standards Board (FASB) issued Accounting Standard Update (ASU)
No. 2014-09, “Revenue from Contracts with Customers (Topic 606)” (ASU 2014-09) as modified by ASU
No. 2015-14, “Revenue from Contracts with Customers (Topic 606): Deferral of the Effective Date.” ASU 2014-
09 will supersede existing revenue recognition standards with a single model unless those contracts are within the
scope of other standards (e.g., an insurance entity’s insurance contracts). The revenue recognition principle in
ASU 2014-09 is that an entity should recognize revenue to depict the transfer of goods or services to customers
in an amount that reflects the consideration to which the entity expects to be entitled in exchange for those goods
or services. In addition, new and enhanced disclosures will be required. Companies can adopt the new standard
either using the full retrospective approach, a modified retrospective approach with practical expedients, or a
cumulative effect upon adoption approach. ASU 2014-09 is effective for annual and interim reporting periods
beginning after December 15, 2017. Early adoption at the original effective date, for interim and annual periods
beginning after December 15, 2016, will be permitted. The Company is currently evaluating the effect of the new
revenue recognition guidance.
In November 2015, the FASB issued ASU No. 2015-17, “Balance Sheet Classification of Deferred Taxes (Topic
740)” (ASU 2015-17). ASU 2015-17 requires entities to present deferred tax assets and deferred tax liabilities as
noncurrent on a classified balance sheet. ASU -2015-17 is effective for annual and interim reporting periods after
69