United Healthcare 2013 Annual Report Download - page 57
Download and view the complete annual report
Please find page 57 of the 2013 United Healthcare annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
-
21
-
22
-
23
-
24
-
25
-
26
-
27
-
28
-
29
-
30
-
31
-
32
-
33
-
34
-
35
-
36
-
37
-
38
-
39
-
40
-
41
-
42
-
43
-
44
-
45
-
46
-
 47
47 -
 48
48 -
 49
49 -
 50
50 -
 51
51 -
 52
52 -
 53
53 -
 54
54 -
 55
55 -
 56
56 -
 57
57 -
 58
58 -
 59
59 -
 60
60 -
 61
61 -
 62
62 -
 63
63 -
 64
64 -
 65
65 -
 66
66 -
 67
67 -
68
-
69
-
70
-
71
-
72
-
73
-
74
-
75
-
76
-
77
-
78
-
79
-
80
-
81
-
82
-
83
-
84
-
85
-
86
-
87
-
88
-
89
-
90
-
91
-
92
-
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
-
114
-
115
-
116
-
117
-
118
-
119
-
120
 |
 |
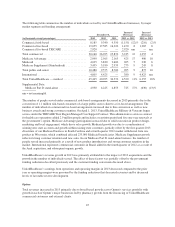
Our Medicare Advantage and Medicare Part D premium revenues are subject to periodic adjustment under CMS’
risk adjustment payment methodology. The CMS risk adjustment model provides higher per member payments
for enrollees diagnosed with certain conditions and lower payments for enrollees who are healthier. We and
health care providers collect, capture, and submit available diagnosis data to CMS within prescribed deadlines.
CMS uses submitted diagnosis codes, demographic information, and special statuses to determine the risk score
for most Medicare Advantage beneficiaries. CMS also retroactively adjusts risk scores during the year based on
additional data. We estimate risk adjustment revenues based upon the data submitted and expected to be
submitted to CMS. As a result of the variability of factors that determine such estimations, the actual amount of
CMS’ retroactive payments could be materially more or less than our estimates. This may result in favorable or
unfavorable adjustments to our Medicare premium revenue and, accordingly, our profitability. Risk adjustment
data for certain of our plans is subject to review by the federal and state governments, including audit by
regulators. See Note 12 of Notes to the Consolidated Financial Statements included in Item 8, “Financial
Statements” for additional information regarding these audits. Additionally, beginning in 2014, Medicare
Advantage and Medicare Part D plans will be subject to a minimum MLR threshold of 85%. We will include in
our estimates of premiums to be recognized the expected premium minimum MLR rebates, if any.
U.S. commercial health plans with MLRs on fully insured products, as calculated under the definitions in Health
Reform Legislation, that fall below certain targets (85% for large employer groups, 80% for small employer
groups and 80% for individuals) are required to rebate ratable portions of their premiums to their customers
annually. Premium revenues are recognized based on the estimated premiums earned net of projected rebates
because we are able to reasonably estimate the ultimate premiums of these contracts. Each period, we estimate
premium rebates based on the expected financial performance of the applicable contracts within each defined
aggregation set (e.g., by state, group size and licensed subsidiary). The most significant factors in estimating the
financial performance are current and future premiums and medical claim experience, effective tax rates and
expected changes in business mix. The estimated ultimate premium is revised each period to reflect current and
projected experience.
Goodwill and Intangible Assets
Goodwill. Goodwill represents the amount of the purchase price in excess of the fair values assigned to the
underlying identifiable net assets of acquired businesses. Goodwill is not amortized, but is subject to an annual
impairment test. Impairment tests are performed more frequently if events occur or circumstances change that
would more likely than not reduce the fair value of the reporting unit below its carrying amount.
To determine whether goodwill is impaired, we perform a multi-step impairment test. First, we can elect to
perform a qualitative assessment of each reporting unit to determine whether facts and circumstances support a
determination that their fair values are greater than their carrying values. If the qualitative analysis is not
conclusive, or if we elect to proceed directly with quantitative testing, we will then measure the fair values of the
reporting units and compare them to their aggregate carrying values, including goodwill. If the fair value is less
than the carrying value of the reporting unit, then the implied value of goodwill would be calculated and
compared to the carrying amount of goodwill to determine whether goodwill is impaired.
We estimate the fair values of our reporting units using discounted cash flows, which include assumptions about
a wide variety of internal and external factors. Significant assumptions used in the impairment analysis include
financial projections of free cash flow (including significant assumptions about operations, capital requirements
and income taxes), long-term growth rates for determining terminal value beyond the discretely forecasted
periods, and discount rates. For each reporting unit, comparative market multiples are used to corroborate the
results of our discounted cash flow test.
55