United Healthcare 2002 Annual Report Download - page 35
Download and view the complete annual report
Please find page 35 of the 2002 United Healthcare annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
-
21
-
22
-
23
-
24
-
 25
25 -
 26
26 -
 27
27 -
 28
28 -
 29
29 -
 30
30 -
 31
31 -
 32
32 -
 33
33 -
 34
34 -
 35
35 -
 36
36 -
 37
37 -
 38
38 -
 39
39 -
 40
40 -
 41
41 -
 42
42 -
 43
43 -
 44
44 -
 45
45 -
46
-
47
-
48
-
49
-
50
-
51
-
52
-
53
-
54
-
55
-
56
-
57
-
58
-
59
-
60
-
61
-
62
-
63
-
64
-
65
-
66
-
67
 |
 |

{ 34 }
UnitedHealth Group
REGULATORY CAPITAL AND DIVIDEND RESTRICTIONS
We conduct a significant portion of our operations through companies that are subject to standards
established by the National Association of Insurance Commissioners (NAIC). These standards, among other
things, require these subsidiaries to maintain specified levels of statutory capital, as defined by each state, and
restrict the timing and amount of dividends and other distributions that may be paid to their parent
companies. Generally, the amount of dividend distributions that may be paid by a regulated subsidiary,
without prior approval by state regulatory authorities, is limited based on the entity’s level of statutory net
income and statutory capital and surplus. The agencies that assess our creditworthiness also consider capital
adequacy levels when establishing our debt ratings. Consistent with our intent to maintain our senior debt
ratings in the “A” range, we maintain an aggregate statutory capital level for our regulated subsidiaries that is
significantly higher than the minimum level regulators require. As of December 31, 2002, our regulated
subsidiaries had aggregate statutory capital of approximately $2.5 billion, which is significantly more than the
aggregate minimum regulatory requirements.
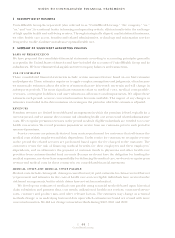
CRITICAL ACCOUNTING POLICIES AND ESTIMATES
Critical accounting policies are those policies that require management to make the most challenging,
subjective or complex judgments, often because they must estimate the effects of matters that are
inherently uncertain and may change in subsequent periods. Critical accounting policies involve
judgments and uncertainties that are sufficiently sensitive to result in materially different results under
different assumptions and conditions. We believe our most critical accounting policies are those
described below. For a detailed discussion of these and other accounting policies, see Note 2 to the
Consolidated Financial Statements.
REVENUES
Revenues are principally derived from health care insurance premiums. We recognize premium revenues
in the period eligible individuals are entitled to receive health care services. Customers are typically billed
monthly at a contracted rate per eligible person multiplied by the total number of people eligible to
receive services, as recorded in our records. Employer groups generally provide us with changes to their
eligible population one month in arrears. Each billing includes an adjustment for prior month changes in
eligibility status that were not reflected in our previous billing. We estimate and adjust the current period’s
revenues and accounts receivable accordingly. Our estimates are based on historical trends, premiums
billed, the level of contract renewal activity and other relevant information. We also estimate the amount
of uncollectible receivables each period and record valuation allowances based on historical collection
rates, the age of unpaid amounts, and information about the creditworthiness of the customers. We revise
estimates of revenue adjustments and uncollectible accounts receivable each period, and record changes
in the period they become known.