HCA Holdings 2012 Annual Report Download - page 10
Download and view the complete annual report
Please find page 10 of the 2012 HCA Holdings annual report below. You can navigate through the pages in the report by either clicking on the pages listed below, or by using the keyword search tool below to find specific information within the annual report.-
 1
1 -
 2
2 -
 3
3 -
 4
4 -
 5
5 -
 6
6 -
 7
7 -
 8
8 -
 9
9 -
 10
10 -
 11
11 -
 12
12 -
 13
13 -
 14
14 -
 15
15 -
 16
16 -
 17
17 -
 18
18 -
 19
19 -
 20
20 -
 21
21 -
22
-
23
-
24
-
25
-
26
-
27
-
28
-
29
-
30
-
31
-
32
-
33
-
34
-
35
-
36
-
37
-
38
-
39
-
40
-
41
-
42
-
43
-
44
-
45
-
46
-
47
-
48
-
49
-
50
-
51
-
52
-
53
-
54
-
55
-
56
-
57
-
58
-
59
-
60
-
61
-
62
-
63
-
64
-
65
-
66
-
67
-
68
-
69
-
70
-
71
-
72
-
73
-
74
-
75
-
76
-
77
-
78
-
79
-
80
-
81
-
82
-
83
-
84
-
85
-
86
-
87
-
88
-
89
-
90
-
91
-
92
-
93
-
94
-
95
-
96
-
97
-
98
-
99
-
100
-
101
-
102
-
103
-
104
-
105
-
106
-
107
-
108
-
109
-
110
-
111
-
112
-
113
-
114
-
115
-
116
-
117
-
118
-
119
-
120
-
121
-
122
-
123
-
124
-
125
-
126
-
127
-
128
-
129
-
130
-
131
-
132
-
133
-
134
-
135
-
136
-
137
-
138
-
139
-
140
-
141
-
142
-
143
-
144
-
145
-
146
-
147
-
148
-
149
-
150
-
151
-
152
-
153
-
154
-
155
-
156
-
157
-
158
-
159
-
160
-
161
 |
 |

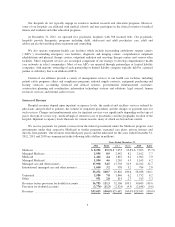
Medicare is a federal program that provides certain hospital and medical insurance benefits to persons
age 65 and over, some disabled persons, persons with end-stage renal disease and persons with Lou Gehrig’s
Disease. Medicaid is a federal-state program, administered by the states, which provides hospital and medical
benefits to qualifying individuals who are unable to afford health care. All of our general, acute care hospitals
located in the United States are eligible to participate in Medicare and Medicaid programs. Amounts received
under Medicare and Medicaid programs are generally significantly less than established hospital gross charges
for the services provided.
Our hospitals generally offer discounts from established charges to certain group purchasers of health care
services, including private insurance companies, employers, health maintenance organizations (“HMOs”),
preferred provider organizations (“PPOs”) and other managed care plans. These discount programs generally
limit our ability to increase revenues in response to increasing costs. See Item 1, “Business — Competition.”
Patients are generally not responsible for the total difference between established hospital gross charges and
amounts reimbursed for such services under Medicare, Medicaid, HMOs, PPOs and other managed care plans,
but are responsible to the extent of any exclusions, deductibles or coinsurance features of their coverage. The
amount of such exclusions, deductibles and coinsurance continues to increase. Collection of amounts due from
individuals is typically more difficult than from governmental or third-party payers. We provide discounts to
uninsured patients who do not qualify for Medicaid or charity care under our charity care policy. These discounts
are similar to those provided to many local managed care plans. In implementing the uninsured discount policy,
we attempt to qualify uninsured patients for Medicaid, other federal or state assistance or charity care under our
charity care policy. If an uninsured patient does not qualify for these programs, the uninsured discount is applied.
Medicare
In addition to the reimbursement reductions and adjustments discussed below, the Budget Control Act of
2011 (the “BCA”) requires automatic spending reductions beginning in 2013 to reduce the federal deficit,
including Medicare spending reductions of up to 2% for a fiscal year, with a uniform percentage reduction across
all Medicare programs. The President and Congress continue to negotiate federal government spending
reductions, but if no action is taken by March 1, 2013, the BCA-mandated spending reductions will occur. It is
unclear how these reductions will be implemented across the different Medicare payment systems discussed
below or whether any negotiations will result in different spending reductions or a temporary delay.
Inpatient Acute Care
Under the Medicare program, we receive reimbursement under a prospective payment system (“PPS”) for
general, acute care hospital inpatient services. Under the hospital inpatient PPS, fixed payment amounts per
inpatient discharge are established based on the patient’s assigned Medicare severity diagnosis-related group
(“MS-DRG”). MS-DRGs classify treatments for illnesses according to the estimated intensity of hospital
resources necessary to furnish care for each principal diagnosis. MS-DRG weights represent the average
resources for a given MS-DRG relative to the average resources for all MS-DRGs. MS-DRG payments are
adjusted for area wage differentials. Hospitals, other than those defined as “new,” receive PPS reimbursement for
inpatient capital costs based on MS-DRG weights multiplied by a geographically adjusted federal rate. When the
cost to treat certain patients falls well outside the normal distribution, providers typically receive additional
“outlier” payments.
MS-DRG rates are updated, and MS-DRG weights are recalibrated, using cost-relative weights each federal
fiscal year (which begins October 1). The index used to update the MS-DRG rates (the “market basket”) gives
consideration to the inflation experienced by hospitals and entities outside the health care industry in purchasing
goods and services. The Patient Protection and Affordable Care Act, as amended by the Health Care and
Education Reconciliation Act of 2010 (collectively, the “Health Reform Law”), provides for annual decreases to
the market basket, including the following reductions for each of the following federal fiscal years: 0.1% in
2013; 0.3% in 2014; 0.2% in 2015 and 2016 and 0.75% in 2017, 2018 and 2019. For federal fiscal year 2012 and
6